|
|
Abstract: ASN Annual Meeting 2020 -- Digital Meeting |
Knauf F, Grujic D, Keddis MT, et al.

Pharmacodynamic (PD) Profiling of Reloxaliase in Patients with Severe Hyperoxaluria
ASN Annual Meeting 2020 -- Digital Meeting
J Am Soc Nephrol (Oct) 31:6A 2020
BACKGROUND
Hyperoxaluria is a major risk factor for kidney stones and can lead to chronic kidney disease (CKD). With decreasing kidney function, plasma oxalate (POx) rises and oxalate may deposit in the kidneys and other tissues (systemic oxalosis) leading to ESRD. Reloxaliase (REL), a non-absorbed, oxalate specific oral enzyme therapy designed to degrade oxalate along the GI tract, may potentially reduce the systemic and renal oxalate burden in patients with enteric and primary hyperoxaluria (EH and PH). This study tested the PD of REL, and addressed questions regarding potential formate accumulation (by-product of oxalate degradation) and systemic absorption of oxalate decarboxilase (OxDc, the active component of REL).
METHODS
This 12-week, open label study enrolled subjects with EH, CKD and hyperoxalemia (UOx ≥40mg/d, eGFR <45mL/min and POx>5μmol/L, n=10) and PH (UOx ≥40 mg/d, n=5) who received 7,500u of REL 5x/day with meals/snacks. Parameters assessed at baseline, and weeks 4, 8 and 12 included POx and UOx (only if eGFR >15mL/min), plasma formic acid (pre- and post-prandial/post-dose; Q2 Solutions) and OxDc (specific ELISA, Absorption Systems).
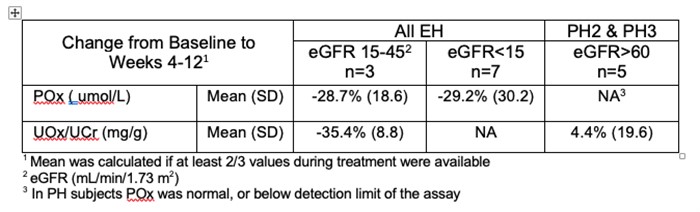
RESULTS
Reported adverse events (AEs) were mostly GI related; there were no related serious AEs. In EH, both POx and UOx decreased substantially; in PH, UOx did not change, and POx stayed normal at baseline and during treatment (Table). There was no formate accumulation, as all samples were below or within normal range (1- 9mg/L). Similarly, there was no detectable absorption of REL, as all samples were below the limit of detection of the assay for OxDc (<0.0001% of the administered dose of 37,500 u/day).
CONCLUSION
Reloxaliase was well tolerated; the absence of formate accumulation further supports its safety. The lack of REL absorption, in addition to supporting low potential for systemic toxicity, confirms its site of action within the GI tract. This best aligns with the pathophysiology of EH as evidenced by the substantial reduction in both POx and UOx in EH subjects with CKD/ESRD.
c Copyright 2020 -2021 American Society of Nephrology. Reproduced with permission.
All ASN abstracts from the 2020 Annual Meeting are available at this link and also are archived in .pdf form at ASN-Online.org
Disclaimer: Abstracts often have errors, both typographical and otherwise. This posting is an electronic translation of submitted abstracts which has not been verified against the original submitted abstract nor with the authors for accuracy. As a result, there may be errors, especially with regard to drug doses, but not limited to these. Abstracts undergo only limited review, and data often are changed as a result of the peer review process, so their reliability is less than manuscripts published in peer-reviewed journals. In using these summaries, you are agreeing that you are aware of these limitations.
The materials are provided on an as-is basis without any warranty of any kind, either express or implied. In addition to errors, the information presented may be incomplete or outdated. The information contained is not intended nor recommended as a substitute for professional medical advice. You are advised to check the appropriate medical literature and the product information currently provided by the manufacturer of each device to be used or drug to be administered to verify the dosage, the method and duration of administration, or contraindications. It is the responsibility of the treating physician or other health care professional, relying on independent experience and knowledge of the patient, to determine drug, disease, and the best treatment for the patient.
To the fullest extent permitted by law, HDCN, ASN and their affiliates and suppliers disclaim all warranties, express or implied, including, but not limited to, any warranty of merchantability, non- infringement or fitness for a particular purpose.
In no event shall HDCN, ASN, or their affiliates or suppliers be liable for any damages whatsoever (including, but not limited to, direct, indirect, incidental, consequential, punitive or exemplary damages, or any damages for loss of profits, use, data, goodwill or other intangibles) arising from or in any way relating to these terms, the materials, or any information, goods or services obtained from or referred to in the materials, whether based on warranty, contract, tort (including, but not limited to, negligence), or any other legal theory, and whether or not any or all of the limited entities is advised of the possibility of such damages.
Related Folders: